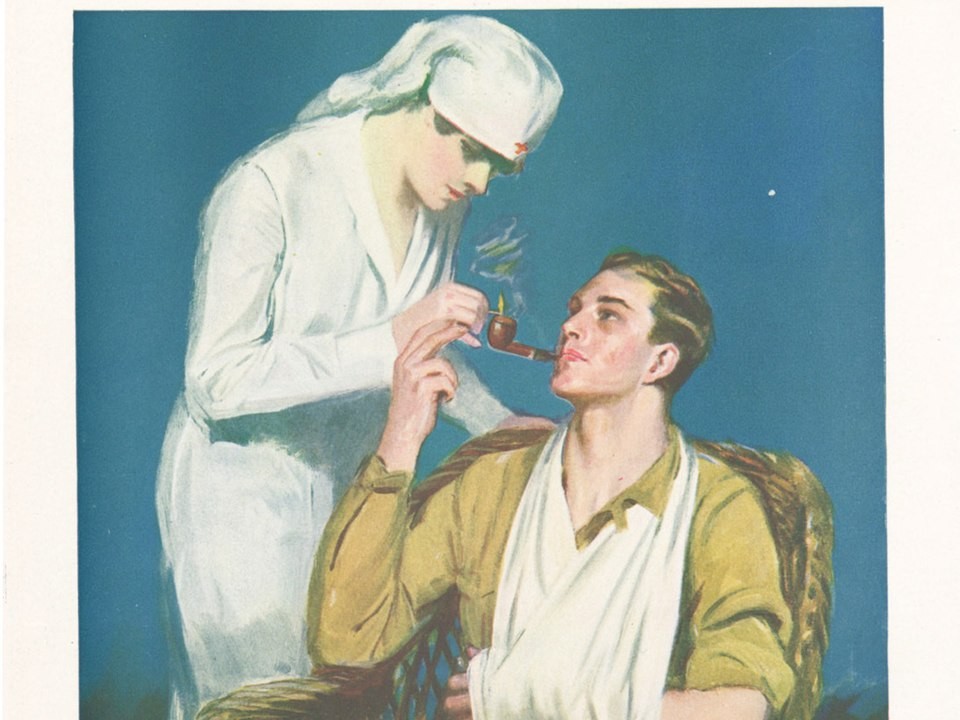
Mid-century cigarette ads did more than sell tobacco. They sold emotional safety through white coats, calm language, and the suggestion that modern medicine had already weighed the risks. For many families, that framing felt rational, even responsible. The message was simple: if trusted professionals seemed comfortable, ordinary people could relax too.
The historical record shows this was not a fringe tactic. A widely cited public health analysis documents how tobacco brands used physicians heavily in U.S. advertising from 1930 to 1953, including campaigns built around survey-style claims about doctors’ preferences.
At the same time, scientific evidence linking smoking and lung disease was already accumulating in major journals. In 1950, Wynder and Graham published their 684-case study in JAMA, and Doll and Hill published their preliminary report in BMJ the same year.
What failed was not only product safety. What failed was a trust system: experts, publishers, marketers, and regulators moving at different speeds while the public assumed they were moving together. That gap between appearance and reality became the real public health lesson, and it still matters whenever commercial messaging borrows scientific authority.
The White Coat as a Marketing Shortcut

A physician in an advertisement communicates more than technical knowledge. It signals care, duty, and restraint. In the 1950s ad ecosystem, that symbolism gave cigarette copy a credibility boost that ordinary testimonials could not match. It turned a consumption choice into something that looked medically vetted.
Archival research shows these campaigns were not accidental one-offs. Tobacco firms repeatedly designed ads that used doctors and medical language to reassure smokers, often implying broad clinical approval without providing the kind of evidence modern audiences would expect.
The structure of those ads was clever. They rarely argued, they implied. They leaned on tone, repetition, and selective framing, then let readers fill in the rest. That is exactly how trust gets moved at scale, quietly and efficiently.
The deeper issue is that symbols can outrun science. Once a white coat enters a commercial frame, people tend to read certainty where only marketing intent exists. When that happens repeatedly, critical judgment becomes a social tax that too few people can pay in real time.
Evidence Was Emerging While Reassurance Stayed Loud
By 1950, concern about smoking and lung cancer had already moved into major medical discourse. Wynder and Graham’s JAMA publication and Doll and Hill’s BMJ report are central landmarks in that shift, even if many consumers never saw those papers directly.
Industry messaging, however, did not pause while evidence matured. Public-facing reassurance remained highly visible, and that visibility created its own reality for households that trusted familiar brands more than distant journals.
This mismatch in speed mattered. Scientific confidence usually builds through replication, argument, and revision. Advertising confidence arrives prepackaged, with a slogan and a deadline. The two systems were never designed to compete on equal terms.
By 1964, the first Surgeon General report had reviewed more than 7,000 articles and concluded cigarette smoking caused major harms, including lung cancer in men and chronic bronchitis, which marked a major federal acknowledgment of the risk picture.
Institutions Helped Normalize the Signal Before Pulling Back
Public trust did not hinge on ads alone. It also depended on where those messages appeared and how closely they sat beside professional medicine. Placement can function like endorsement, even when no explicit endorsement is stated.
Historical accounts show tobacco companies actively courted physicians through conventions, office outreach, complimentary cigarettes, and selective scientific materials. That blurred the line between professional culture and commercial influence in ways that were hard for the public to see.
Then the tone shifted. In 1953, JAMA stopped accepting cigarette advertisements and barred cigarette exhibits at AMA conventions, reflecting rising concern within organized medicine about credibility and ethics.
This reversal is important because it reveals timing. Institutions did respond, but after years in which the earlier signal had already shaped habits and beliefs. Trust, once granted at scale, does not unwind on command.
From Doctor Endorsement to Managed Doubt
As direct health reassurance became harder to defend, strategy evolved. Rather than proving cigarettes safe, industry communication increasingly framed the science as unsettled and incomplete, keeping the public in a state of suspended judgment.
Historical analyses describe a coordinated shift in the early 1950s, including high-level meetings with public relations leadership, the creation of the Tobacco Industry Research Committee, and the full-page Frank Statement campaign run across hundreds of newspapers.
That move changed the information battlefield. The goal was no longer simple endorsement. The goal was to normalize uncertainty, recast strong evidence as debate, and preserve consumer confidence long enough to protect sales.
This matters beyond tobacco history. Manufactured ambiguity can be more durable than a direct false claim, because it asks people to postpone decisions rather than reject facts. In practice, postponement often functions as consent.
The Low-Tar Era Extended the Trust Problem
Once obvious doctor-centered reassurance lost force, product differentiation took over. Tar and nicotine metrics became marketing tools, and numbers created a fresh aura of precision for consumers searching for safer choices.
Regulatory records and historical reviews show that the FTC challenged unsupported claims in the 1950s, issued advertising guides in 1955, and later struggled with comparability issues that fed the so-called tar derby before standardized machine methods took hold.
But machine outputs and human behavior were never the same thing. Smokers could inhale differently, compensate with deeper puffs, or smoke more, weakening the protective interpretation of low machine yields.
The National Cancer Institute now states clearly that low-tar cigarettes are no safer than regular cigarettes, and cigarettes are no longer allowed to be labeled or advertised as low tar.
Regulation Eventually Moved, Trust Damage Stayed
Federal action did become stronger over time. Congress enacted major tobacco laws in 1965 and 1969 that required warning labels and banned cigarette advertising in broadcast media, reshaping the public information environment.
Those steps mattered and helped reduce harm over the long run. But regulation can remove messaging channels faster than it repairs beliefs formed over decades. A legal correction is not the same as a cultural reset.
People do not store policy timelines in memory. They store impressions: what authority looked like, who seemed calm, and what felt normal in the room. That is why trust failures can outlast the campaigns that created them.
The long arc of tobacco control proves a hard truth. Public health wins are possible, but recovery takes sustained effort across science communication, policy, education, and institutional accountability, not one headline moment.
What This Teaches About Public Trust Today

This history is not just about the past; it is about governance of credibility. When commercial speech borrows expert symbols, institutions must act early and clearly, or silence gets interpreted as approval.
It also shows that evidence alone is not enough. People make decisions through culture, habit, and social proof. If accurate science is less legible than polished messaging, misinformation can thrive even without explicit lies.
Editorial independence is part of public health infrastructure. Clear conflict rules, transparent funding disclosures, and fast corrections are not bureaucratic extras. They are trust protections that prevent credibility from being rented by the highest bidder.
Most of all, the period demonstrates that trust is a public resource, not a private marketing asset. Once diluted, every later warning sounds less certain than it should. Rebuilding it requires fewer theatrics and more disciplined honesty.
How a Better Trust System Could Work
A stronger model begins with separation. Advertising, clinical guidance, and peer-reviewed evidence should stay visibly distinct so that audiences can tell persuasion from evaluation at a glance.
Second, uncertainty should be communicated precisely, not theatrically. Real uncertainty has boundaries and probabilities. Manufactured uncertainty has slogans. Institutions need to teach that difference repeatedly and in plain language.
Third, regulators and professional bodies should coordinate faster when evidence shifts. The public should not need a decade to learn that the old reassurance model was wrong. Lag time is where avoidable harm accumulates.
Finally, accountability needs memory. Public communication should record who claimed what, when, and on what evidence. That archive discipline makes future trust less vulnerable to recycled narratives dressed up as new confidence.
Sources
- CDC: A History of the Surgeon General’s Reports on Smoking and Health
- AJPH/PMC: The Physician in U.S. Cigarette Advertisements, 1930–1953
- PubMed: Wynder & Graham (1950), 684 Proven Cases
- PubMed: Doll & Hill (1950), Preliminary Report
- NCI Dictionary: Low Tar Cigarette
- NCI Monograph: Cigarette Testing and the Federal Trade Commission

